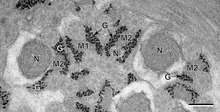
Schematic two-dimensional cross-sectional view of glycogen: A core protein of glycogenin is surrounded by branches of glucose units. The entire globular granule may contain around 30,000 glucose units.[1]A view of the atomic structure of a single branched strand of glucose units in a glycogen molecule.Glycogen (black granules) in spermatozoa of a flatworm; transmission electron microscopy, scale: 0.3 μm
Glycogen is a multibranched polysaccharide of glucose that serves as a form of energy storage in animals,[2]fungi, and bacteria.[3] It is the main storage form of glucose in the human body.
Glycogen functions as one of three regularly used forms of energy reserves, creatine phosphate being for very short-term, glycogen being for short-term and the triglyceride stores in adipose tissue (i.e., body fat) being for long-term storage. Protein, broken down into amino acids, is seldom used as a main energy source except during starvation and glycolytic crisis (see bioenergetic systems).
In humans, glycogen is made and stored primarily in the cells of the liver and skeletal muscle.[4][5] In the liver, glycogen can make up 5–6% of the organ's fresh weight: the liver of an adult, weighing 1.5 kg, can store roughly 100–120 grams of glycogen.[4][6] In skeletal muscle, glycogen is found in a low concentration (1–2% of the muscle mass): the skeletal muscle of an adult weighing 70 kg stores roughly 400 grams of glycogen.[4] Small amounts of glycogen are also found in other tissues and cells, including the kidneys, red blood cells,[7][8][9]white blood cells,[10] and glial cells in the brain.[11] The uterus also stores glycogen during pregnancy to nourish the embryo.[12]
The amount of glycogen stored in the body mostly depends on oxidative type 1 fibres,[13][14] physical training, basal metabolic rate, and eating habits.[15] Different levels of resting muscle glycogen are reached by changing the number of glycogen particles, rather than increasing the size of existing particles[14] though most glycogen particles at rest are smaller than their theoretical maximum.[16]
Approximately 4 grams of glucose are present in the blood of humans at all times;[4] in fasting individuals, blood glucose is maintained constant at this level at the expense of glycogen stores, primarily from the liver (glycogen in skeletal muscle is mainly used as an immediate source of energy for that muscle rather than being used to maintain physiological blood glucose levels).[4] Glycogen stores in skeletal muscle serve as a form of energy storage for the muscle itself;[4] however, the breakdown of muscle glycogen impedes muscle glucose uptake from the blood, thereby increasing the amount of blood glucose available for use in other tissues.[4] Liver glycogen stores serve as a store of glucose for use throughout the body, particularly the central nervous system.[4] The human brain consumes approximately 60% of blood glucose in fasted, sedentary individuals.[4]
Glycogen is an analogue of starch, a glucose polymer that functions as energy storage in plants. It has a structure similar to amylopectin (a component of starch), but is more extensively branched and compact than starch. Both are white powders in their dry state. Glycogen is found in the form of granules in the cytosol/cytoplasm in many cell types, and plays an important role in the glucose cycle. Glycogen forms an energy reserve that can be quickly mobilized to meet a sudden need for glucose, but one that is less compact than the energy reserves of triglycerides (lipids). As such it is also found as storage reserve in many parasitic protozoa.[17][18][19]
Structure
α(1→4)-glycosidic linkages in the glycogen oligomerα(1→4)-glycosidic and α(1→6)-glycosidic linkages in the glycogen oligomer
Glycogen is a branched biopolymer consisting of linear chains of glucoseresidues with an average chain length of approximately 8–12 glucose units and 2,000-60,000 residues per one molecule of glycogen.[20][21]
Like amylopectin, glucose units are linked together linearly by α(1→4) glycosidic bonds from one glucose to the next. Branches are linked to the chains from which they are branching off by α(1→6) glycosidic bonds between the first glucose of the new branch and a glucose on the stem chain.[22]
Each glycogen is essentially a ball of glucose trees, with around 12 layers, centered on a glycogenin protein, with three kinds of glucose chains: A, B, and C. There is only one C-chain, attached to the glycogenin. This C-chain is formed by the self-glucosylation of the glycogenin, forming a short primer chain. From the C-chain grows out B-chains, and from B-chains branch out B- and A-chains. The B-chains have on average 2 branch points, while the A-chains are terminal, thus unbranched. On average, each chain has length 12, tightly constrained to be between 11 and 15. All A-chains reach the spherical surface of the glycogen.[23][24]
Glycogen in muscle, liver, and fat cells is stored in a hydrated form, composed of three or four parts of water per part of glycogen associated with 0.45 millimoles (18 mg) of potassium per gram of glycogen.[5]
Glucose is an osmotic molecule, and can have profound effects on osmotic pressure in high concentrations possibly leading to cell damage or death if stored in the cell without being modified.[3] Glycogen is a non-osmotic molecule, so it can be used as a solution to storing glucose in the cell without disrupting osmotic pressure.[3]
Functions
Liver
As a meal containing carbohydrates or protein is eaten and digested, blood glucose levels rise, and the pancreas secretes insulin. Blood glucose from the portal vein enters liver cells (hepatocytes). Insulin acts on the hepatocytes to stimulate the action of several enzymes, including glycogen synthase. Glucose molecules are added to the chains of glycogen as long as both insulin and glucose remain plentiful. In this postprandial or "fed" state, the liver takes in more glucose from the blood than it releases.
After a meal has been digested and glucose levels begin to fall, insulin secretion is reduced, and glycogen synthesis stops. When it is needed for energy, glycogen is broken down and converted again to glucose. Glycogen phosphorylase is the primary enzyme of glycogen breakdown. For the next 8–12 hours, glucose derived from liver glycogen is the primary source of blood glucose used by the rest of the body for fuel.
Glucagon, another hormone produced by the pancreas, in many respects serves as a countersignal to insulin. In response to insulin levels being below normal (when blood levels of glucose begin to fall below the normal range), glucagon is secreted in increasing amounts and stimulates both glycogenolysis (the breakdown of glycogen) and gluconeogenesis (the production of glucose from other sources).
Muscle
Metabolism of common monosaccharides
Muscle glycogen appears to function as a reserve of quickly available phosphorylated glucose, in the form of glucose-1-phosphate, for muscle cells. Glycogen contained within skeletal muscle cells are primarily in the form of β particles.[25] Other cells that contain small amounts use it locally as well. As muscle cells lack glucose-6-phosphatase, which is required to pass glucose into the blood, the glycogen they store is available solely for internal use and is not shared with other cells. This is in contrast to liver cells, which, on demand, readily do break down their stored glycogen into glucose and send it through the blood stream as fuel for other organs.[26]
Skeletal muscle needs ATP (provides energy) for muscle contraction and relaxation, in what is known as the sliding filament theory. Skeletal muscle relies predominantly on glycogenolysis for the first few minutes as it transitions from rest to activity, as well as throughout high-intensity aerobic activity and all anaerobic activity.[27] During anaerobic activity, such as weightlifting and isometric exercise, the phosphagen system (ATP-PCr) and muscle glycogen are the only substrates used as they do not require oxygen nor blood flow.[27]
Different bioenergetic systems produce ATP at different speeds, with ATP produced from muscle glycogen being much faster than fatty acid oxidation.[28] The level of exercise intensity determines how much of which substrate (fuel) is used for ATP synthesis also. Muscle glycogen can supply a much higher rate of substrate for ATP synthesis than blood glucose. During maximum intensity exercise, muscle glycogen can supply 40 mmol glucose/kg wet weight/minute,[29] whereas blood glucose can supply 4 - 5 mmol.[30][4] Due to its high supply rate and quick ATP synthesis, during high-intensity aerobic activity (such as brisk walking, jogging, or running), the higher the exercise intensity, the more the muscle cell produces ATP from muscle glycogen.[31] This reliance on muscle glycogen is not only to provide the muscle with enough ATP during high-intensity exercise, but also to maintain blood glucose homeostasis (that is, to not become hypoglycaemic by the muscles needing to extract far more glucose from the blood than the liver can provide).[30] A deficit of muscle glycogen leads to muscle fatigue known as "hitting the wall" or "the bonk" (see below under glycogen depletion).
Structure Type
In 1999, Meléndez et al claimed that the structure of glycogen is optimal under a particular metabolic constraint model, where the structure was suggested to be "fractal" in nature.[32] However, research by Besford et al[33] used small angle X-ray scattering experiments accompanied by branching theory models to show that glycogen is a randomly hyperbranched polymer nanoparticle. Glycogen is not fractal in nature. This has been subsequently verified by others who have performed Monte Carlo simulations of glycogen particle growth, and shown that the molecular density reaches a maximum near the centre of the nanoparticle structure, not at the periphery (contradicting a fractal structure that would have greater density at the periphery).[34]
History
Glycogen was discovered by Claude Bernard. His experiments showed that the liver contained a substance that could give rise to reducing sugar by the action of a "ferment" in the liver. By 1857, he described the isolation of a substance he called "la matière glycogène", or "sugar-forming substance". Soon after the discovery of glycogen in the liver, M.A. Sanson found that muscular tissue also contains glycogen. The empirical formula for glycogen of (C 6H 10O 5)n was established by August Kekulé in 1858.[35]
Sanson, M. A. "Note sur la formation physiologique du sucre dans l’economie animale." Comptes rendus des seances de l’Academie des Sciences 44 (1857): 1323-5.
Glycogen synthesis is, unlike its breakdown, endergonic—it requires the input of energy. Energy for glycogen synthesis comes from uridine triphosphate (UTP), which reacts with glucose-1-phosphate, forming UDP-glucose, in a reaction catalysed by UTP—glucose-1-phosphate uridylyltransferase. Glycogen is synthesized from monomers of UDP-glucose initially by the protein glycogenin, which has two tyrosine anchors for the reducing end of glycogen, since glycogenin is a homodimer. After about eight glucose molecules have been added to a tyrosine residue, the enzyme glycogen synthase progressively lengthens the glycogen chain using UDP-glucose, adding α(1→4)-bonded glucose to the nonreducing end of the glycogen chain.[36]
The glycogen branching enzyme catalyzes the transfer of a terminal fragment of six or seven glucose residues from a nonreducing end to the C-6 hydroxyl group of a glucose residue deeper into the interior of the glycogen molecule. The branching enzyme can act upon only a branch having at least 11 residues, and the enzyme may transfer to the same glucose chain or adjacent glucose chains.
Glycogen is cleaved from the nonreducing ends of the chain by the enzyme glycogen phosphorylase to produce monomers of glucose-1-phosphate:
Action of glycogen phosphorylase on glycogen
In vivo, phosphorolysis proceeds in the direction of glycogen breakdown because the ratio of phosphate and glucose-1-phosphate is usually greater than 100.[37] Glucose-1-phosphate is then converted to glucose 6 phosphate (G6P) by phosphoglucomutase. A special debranching enzyme is needed to remove the α(1→6) branches in branched glycogen and reshape the chain into a linear polymer. The G6P monomers produced have three possible fates:
G6P can continue on the glycolysis pathway and be used as fuel.
In the liver and kidney, G6P can be dephosphorylated back to glucose by the enzyme glucose 6-phosphatase. This is the final step in the gluconeogenesis pathway.
Clinical relevance
Disorders of glycogen metabolism
The most common disease in which glycogen metabolism becomes abnormal is diabetes, in which, because of abnormal amounts of insulin, liver glycogen can be abnormally accumulated or depleted. Restoration of normal glucose metabolism usually normalizes glycogen metabolism, as well.
In hypoglycemia caused by excessive insulin, liver glycogen levels are high, but the high insulin levels prevent the glycogenolysis necessary to maintain normal blood sugar levels. Glucagon is a common treatment for this type of hypoglycemia.
Long-distance athletes, such as marathon runners, cross-country skiers, and cyclists, often experience glycogen depletion, where almost all of the athlete's glycogen stores are depleted after long periods of exertion without sufficient carbohydrate consumption. This phenomenon is referred to as "hitting the wall" in running and "bonking" in cycling.
Glycogen depletion can be forestalled in three possible ways:
First, during exercise, carbohydrates with the highest possible rate of conversion to blood glucose (high glycemic index) are ingested continuously. The best possible outcome of this strategy replaces about 35% of glucose consumed at heart rates above about 80% of maximum.
Second, through endurance training adaptations and specialized regimens (e.g. fasting, low-intensity endurance training), the body can condition type I muscle fibers to improve both fuel use efficiency and workload capacity to increase the percentage of fatty acids used as fuel,[38][39] sparing carbohydrate use from all sources.
Third, by consuming large quantities of carbohydrates after depleting glycogen stores as a result of exercise or diet, the body can increase storage capacity of intramuscular glycogen stores.[13][40][41][42] This process is known as carbohydrate loading. In general, glycemic index of carbohydrate source does not matter since muscular insulin sensitivity is increased as a result of temporary glycogen depletion.[43][44]
When athletes ingest both carbohydrate and caffeine following exhaustive exercise, their glycogen stores tend to be replenished more rapidly;[45][46] however, the minimum dose of caffeine at which there is a clinically significant effect on glycogen repletion has not been established.[46]
^Sadava, David E.; Purves, William K.; Hillis, David M.; Orians, Gordon H.; Heller, H. Craig (2011). Life (9th ed.). W. H. Freeman. ISBN9781429254311.
^ abcBerg JM, Tymoczko JL, Gatto GJ, Stryer L (8 April 2015). Biochemistry (8th ed.). New York: W. H. Freeman. ISBN9781464126109. OCLC913469736.
^ abcdefghijWasserman DH (January 2009). "Four grams of glucose". American Journal of Physiology. Endocrinology and Metabolism. 296 (1): E11–21. doi:10.1152/ajpendo.90563.2008. PMC2636990. PMID18840763. Four grams of glucose circulates in the blood of a person weighing 70 kg. This glucose is critical for normal function in many cell types. In accordance with the importance of these 4 g of glucose, a sophisticated control system is in place to maintain blood glucose constant. Our focus has been on the mechanisms by which the flux of glucose from liver to blood and from blood to skeletal muscle is regulated. ... The brain consumes ~60% of the blood glucose used in the sedentary, fasted person. ... The amount of glucose in the blood is preserved at the expense of glycogen reservoirs (Fig. 2). In postabsorptive humans, there are ~100 g of glycogen in the liver and ~400 g of glycogen in muscle. Carbohydrate oxidation by the working muscle can go up by ~10 fold with exercise, and yet after 1 h, blood glucose is maintained at ~4 g.
^Miwa I, Suzuki S (November 2002). "An improved quantitative assay of glycogen in erythrocytes". Annals of Clinical Biochemistry. 39 (Pt 6): 612–13. doi:10.1258/000456302760413432. PMID12564847.
^Benchimol, Marlene; Elias, Cezar Antonio; de Souza, Wanderley (December 1982). "Tritrichomonas foetus: Ultrastructural localization of calcium in the plasma membrane and in the hydrogenosome". Experimental Parasitology. 54 (3): 277–284. doi:10.1016/0014-4894(82)90036-4. ISSN0014-4894. PMID7151939.
^Mielewczik, Michael; Mehlhorn, Heinz; al Quraishy, Saleh; Grabensteiner, E.; Hess, M. (1 September 2008). "Transmission electron microscopic studies of stages of histomonas meleagridis from clonal cultures". Parasitology Research. 103 (4): 745–750. doi:10.1007/s00436-008-1009-1. ISSN0932-0113. PMID18626664. S2CID2331300.
^Quinn A. Besford; Xiao-Yi Zeng; Ji-Ming Ye; Angus Gray-Weale (31 October 2015) [31 October 2015]. "Liver glycogen in type 2 diabetic mice is randomly branched as enlarged aggregates with blunted glucose release". Glycoconjugate Journal. 33 (1). 41-51. doi:10.1007/s10719-015-9631-5. hdl:11343/282927. PMID26521055.
^McDonald, Lyle (1998). The Ketogenic Diet: A complete guide for the dieter and the practitioner. Lyle McDonald.
^Costill DL, Bowers R, Branam G, Sparks K (December 1971). "Muscle glycogen utilization during prolonged exercise on successive days". J Appl Physiol. 31 (6): 834–838. doi:10.1152/jappl.1971.31.6.834. PMID5123660.
^Zorzano A, Balon TW, Goodman MN, Ruderman NB (December 1986). "Glycogen depletion and increased insulin sensitivity and responsiveness in muscle after exercise". Am. J. Physiol. 251 (6, Part 1): E664–E669. doi:10.1152/ajpendo.1986.251.6.E664. PMID3538900.
^McDonald, Lyle (2003). The Ultimate Diet 2.0. Lyle McDonald.
^Pedersen, D.J.; Lessard, S.J.; Coffey, V.G.; et al. (July 2008). "High rates of muscle glycogen resynthesis after exhaustive exercise when carbohydrate is coingested with caffeine". Journal of Applied Physiology. 105 (1): 7–13. doi:10.1152/japplphysiol.01121.2007. PMID18467543.
^ abBeelen, M.; Burke, L.M.; Gibala, M.J.; van Loon, L.J.C. (December 2010). "Nutritional strategies to promote post-exercise recovery". International Journal of Sport Nutrition and Exercise Metabolism. 20 (6): 515–532. doi:10.1123/ijsnem.20.6.515. PMID21116024. S2CID13748227.
هذه مقالة غير مراجعة. ينبغي أن يزال هذا القالب بعد أن يراجعها محرر مغاير للذي أنشأها؛ إذا لزم الأمر فيجب أن توسم المقالة بقوالب الصيانة المناسبة. يمكن أيضاً تقديم طلب لمراجعة المقالة في الصفحة المخصصة لذلك. (ديسمبر 2020) يفتقر محتوى هذه المقالة إلى الاستشهاد بمصادر. فضلاً، سا�...
Artikel ini memiliki beberapa masalah. Tolong bantu memperbaikinya atau diskusikan masalah-masalah ini di halaman pembicaraannya. (Pelajari bagaimana dan kapan saat yang tepat untuk menghapus templat pesan ini) Artikel ini membutuhkan rujukan tambahan agar kualitasnya dapat dipastikan. Mohon bantu kami mengembangkan artikel ini dengan cara menambahkan rujukan ke sumber tepercaya. Pernyataan tak bersumber bisa saja dipertentangkan dan dihapus.Cari sumber: IKSPI Kera Sakti – be...
Fornos de AlgodresDatos generalesNombre Associação Desportiva de Fornos de AlgodresFundación 1970Presidente Bruno Filipe Ventura CostaEntrenador Carlos LopesInstalacionesEstadio Municipal de Fornos de AlgodresCapacidad 1,500Ubicación Fornos de Algodres, Distrito de Guarda, Portugal Titular Alternativo Última temporadaLiga AF Guarda 1° Divisão Página web oficial[editar datos en Wikidata] El A.D. Fornos de Algodres es un club de fútbol portugués del municipio de Fornos de Al...
Опис файлу Опис Джерело http://en.wikipedia.org/wiki/File:Elton_John_-_Honky_Château.jpg Автор зображення Ліцензія див. нижче У цього зображення немає: опису інформації про автора Якщо ви маєте таку інформацію чи маєте до неї доступ, будь ласка, додайте її на сторінку опису зображення. Для сповіщення...
Цей файл був автоматично скопійований з Вікісховища через відсутність свободи панорами в Україні та може потребувати: зміну опису файлу та/чи заміну ліцензії заміну використання оригінального файлу File:StatueMother&ChildEupatoria.jpg цією копією. Це зображення було скопійоване з Wiki...
Balgengaszähler mit darüber sitzendem, vorgeschalteten Gasdruckregler Ein Gaszähler (veraltet bzw. umgangssprachlich teilweise als Gasuhr oder Gasmesser bezeichnet) ist ein Messgerät zur Ermittlung einer durchgesetzten Gasmenge. Gaszähler kommen überwiegend in häuslichen und gewerblichen Gasinstallationen zum Einsatz, werden aber auch zur exakten Mengenbestimmung bei labortechnischen Untersuchungen eingesetzt. Die vom Gaszähler erfasste Einheit ist der Kubikmeter im Betriebszustand, d...
Бромон-ЛамотBromont-Lamothe Країна Франція Регіон Овернь-Рона-Альпи Департамент Пюї-де-Дом Округ Ріом Кантон Понжибо Код INSEE 63055 Поштові індекси 63230 Координати 45°50′28″ пн. ш. 2°49′12″ сх. д.H G O Висота 574 - 906 м.н.р.м. Площа 38,07 км² Населення 994 (01-2020[1]) Густота ...
Eublepharidae Tokek kucing(Aeluroscalabotes felinus) Klasifikasi ilmiah Kerajaan: Animalia Filum: Chordata Subfilum: Vertebrata Kelas: Reptilia Ordo: Squamata Subordo: Lacertilia Infraordo: Gekkota Famili: EublepharidaeBoulenger, 1883 Eublepharidae adalah famili tokek yang terdiri dari sekitar 30 spesies yang tersebar luas di daerah tropis Asia, Afrika, dan Amerika Utara bagian selatan. Tokek-tokek ini memiliki kemiripan morfologi dengan jenis-jenis dari Gekkonidae. Akan tetapi, semua spesies...
Опис Плакат до фільму «Міхай Хоробрий» (рум. Mihai Viteazul, Румунія, 1971) Джерело http://www.altcine.com/posters/photo/MichaeltheBravePoster.jpg Час створення невідомо Автор зображення Студія-виробник та/або дистриб'ютор Ліцензія Це зображення є рекламним плакатом фільму, спортивного або іншого заходу. Найі
Youth awards programme founded in the United Kingdom This article is about the award. For the episode of The Inbetweeners titled The Duke of Edinburgh Awards, see List of The Inbetweeners episodes § ep11. The Duke of Edinburgh's AwardDate13 October 1956; 67 years ago (1956-10-13)CountryUnited Kingdom and othersReward(s)Gold, Silver or Bronze (UK)PatronPrince Edward, Duke of Edinburgh[1]Websitewww.dofe.org The Duke of Edinburgh's Award (commonly abbreviated DofE...
2003 American filmG.I. Joe: Spy TroopsDirected byDale CarmanWritten byLarry HamaProduced byDaley MillerSteve DruckerStarringJohn PayneLisa Ann BeleyMichael DobsonScott McNeilMusic byJohn HunterProductioncompaniesReel FX Creative StudiosHasbro EntertainmentDistributed byParamount Home EntertainmentRelease date September 27, 2003 (2003-09-27) Running time45 minutesCountryUnited StatesLanguageEnglish G.I. Joe: Spy Troops is a 2003 American computer-animated military science fictio...
美國海軍作戰部羅伯特·P·布里斯科(英语:Robert P. Briscoe)中將2月2日在五角大楼舉行撤離大陳島的記者會 大陳軍民在海灘上等候登上第七艦隊的船 大陳島軍民在中美聯合艦隊的協助下,移防撤退之情景,攝於1955年。 金剛計劃(英文:Operation King Kong),是由美軍和中華民國國軍合力進行一項軍事計劃,於1955年2月8日開始進行,內容主要是撤退上下大陳、披山、漁山島,將島上...
ليبيركورت شعار الاسم الرسمي (بالفرنسية: Libercourt) الإحداثيات 50°29′02″N 3°00′50″E / 50.483888888889°N 3.0138888888889°E / 50.483888888889; 3.0138888888889[1] [2] تاريخ التأسيس 1947 تقسيم إداري البلد فرنسا[3] التقسيم الأعلى باد كاليه خصائص جغرافية المساحة ...
Beloeil ou Belœil Castelo de Beloeil Beloeil ou BelœilLocalização de Beloeil na Bélgica 50° 33' N 3° 44' E localização do município, no distrito e na província Brasão Bandeira Geografia Região Valônia Província Hainaut Distrito Ath Área 61,55 km² Demografia População– Homens– Mulheres– Densidade 13.380 (01/07/2006)48,99%51,01%217,38 hab./km2 Faixa Etária 0–19 anos 20–64 anos 65 anos ou mais (01/01/2006)23,42%59,98%16,60% Estrangeiros 5,10% (01...
Administrative entry restrictions This article uses bare URLs, which are uninformative and vulnerable to link rot. Please consider converting them to full citations to ensure the article remains verifiable and maintains a consistent citation style. Several templates and tools are available to assist in formatting, such as reFill (documentation) and Citation bot (documentation). (September 2022) (Learn how and when to remove this template message) A Tajik passport Visa requirements for Tajik c...
Local government building in the United States This article includes a list of general references, but it lacks sufficient corresponding inline citations. Please help to improve this article by introducing more precise citations. (June 2018) (Learn how and when to remove this template message) United States historic placeAllen County CourthouseU.S. National Register of Historic Places Allen County Courthouse Main EntranceInteractive map showing the location of Allen County CourthouseLocationL...
Languages of the country and its peoples Languages of UgandaWarning sign in Luganda, English and SwahiliOfficialEnglish and SwahiliNationalEnglishRecognisedSouthern Luo, Lugbara, Runyankole, Lusoga, AtesoVernacularLugandaMinoritymany Bantu and Nilo-Saharan languages; NubiSignedUgandan Sign LanguageKeyboard layoutQWERTYLanguage families map of Uganda In Uganda the most spoken language in the capital city is Luganda, followed by English (also the official language since 1962), as all schoo...
2005 studio album by Toby KeithHonkytonk UniversityStudio album by Toby KeithReleasedMay 17, 2005GenreCountryLength41:22LabelDreamWorks RecordsProducerToby KeithJames StroudToby Keith chronology Greatest Hits 2(2004) Honkytonk University(2005) White Trash with Money(2006) Singles from Honkytonk University Honkytonk UReleased: February 8, 2005 As Good as I Once WasReleased: May 9, 2005 Big Blue NoteReleased: September 5, 2005 Professional ratingsAggregate scoresSourceRatingMetacritic(6...
El Nuevo Día Tipo DiarioFormato tabloidePaís Estados UnidosSede Guaynabo, Puerto RicoFundación 1909 (como El Diario de Puerto Rico)[1]Fundador(a) Guillermo V. Cintrón[1]Eugenio AstolNemesio Canales[2]Idioma EspañolPrecio 55₵Frecuencia diariaPropietario(a) Grupo Ferré-Rangel (GFR Media, LLC)[3]Subdirector(a) Benjamín Morales MeléndezEditor(a) María Luisa Ferré RangelSitio web www.elnuevodia.com[editar datos en Wikidata] El Nuevo Día es el peri...
Kūsen Madōshi Kōhosei no Kyōkan空戦魔導士候補生の教官GéneroAcción, fantasía, harem, sobrenatural, escolar Novela ligeraCreado porYū MoroboshiIlustrado porYuka NakajimaEditorialFujimi ShobōPublicado enFujimi Fantasía BunkoDemografíaSeinenPrimera publicación20 de julio de 2013Última publicación20 de julio de 2017Volúmenes14 Ficha en Anime News Network MangaCreado porArisu ShidōEditorialMedia FactoryPublicado enComic AliveDemografíaSeinenPrimera publicación26 de juli...
Strategi Solo vs Squad di Free Fire: Cara Menang Mudah!








{kind=link}

{kind=link}




{kind=link}






")


")
